The Neurocognitive Theory (TNC), conceived by Prof. Dr. Carlo Cesare Perfetti (1940 – 2020) in the 1970s, studies the recovery of motor organization for subjects suffering from neurological pathologies of central or peripheral origin, pain syndromes, degenerative and musculoskeletal pathologies.
This theory considers that in order to reach advanced movement that brings the patient back to optimal performance, adopting modalities that engage the body and mind in a unitary and integrated way is a necessity.
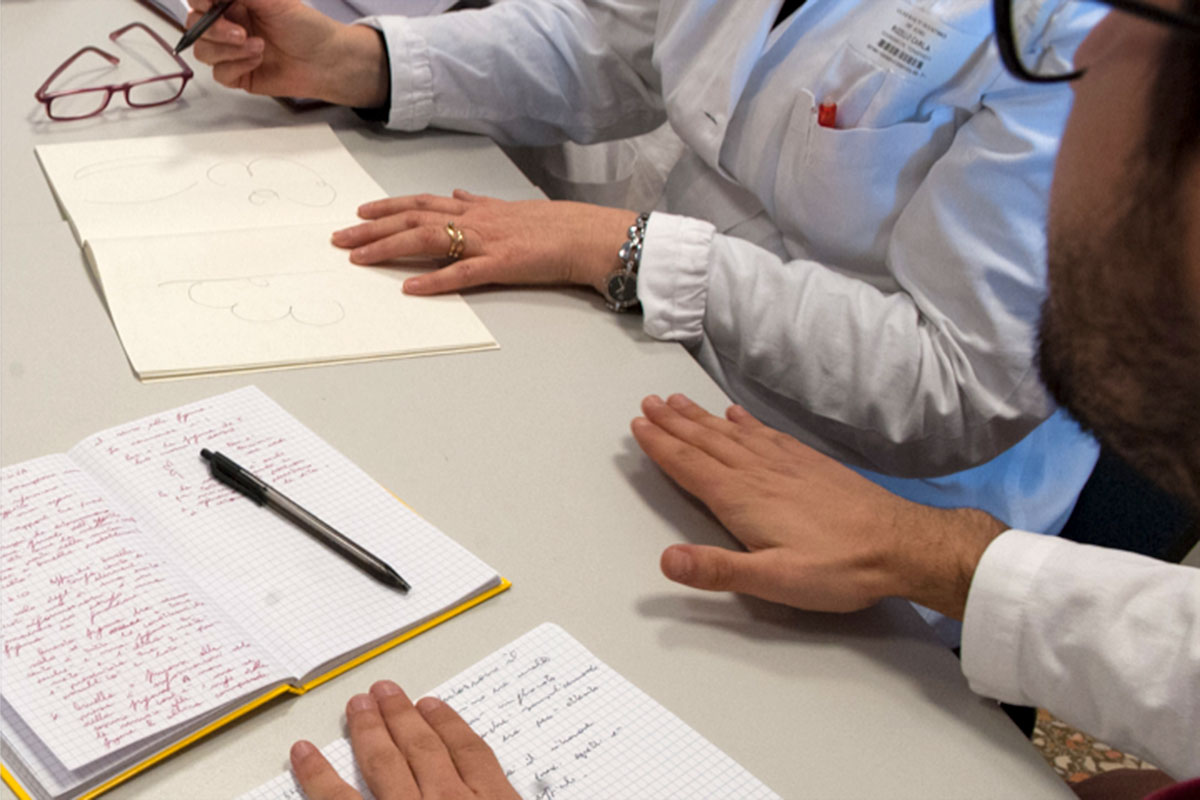
The fundamental premise of Neurocognitive Rehabilitation (RNC) is that the processes of knowledge changes the biological structure of people and their actions, possibly affecting the subject as a whole. The pathology in general (and the neurological one in particular) disrupts the mind-body unit severely. Among the consequences, the subject loses the ability to perceive themselves in their own body, no longer recognizing indispensable self-attributes in interacting with the world.
The original hypothesis of the TNC pertains to the quality of recovery, both spontaneous and guided by the therapist, relying on the activation of cognitive processes and manner of initiation.